Understanding the Condition
What Is Prostatitis?
Prostatitis refers to inflammation or infection of the prostate gland. It is not a single condition — it is a classification covering four distinct categories, each with different causes, presentations, and treatment requirements. Understanding which category you have is the essential first step, because the most common mistake in prostatitis management is treating the wrong type.
The prostate gland sits just below the bladder and surrounds the urethra. When it becomes inflamed or infected, it causes a range of symptoms — pelvic pain, urinary difficulties, pain during or after ejaculation, and in some cases sexual dysfunction. These symptoms can be debilitating and have a significant impact on quality of life.
Prostatitis is the most common urological diagnosis in men under 50 and the third most common in men over 50. Despite its prevalence, it is frequently mismanaged — often because GPs and non-specialist practitioners apply a one-size-fits-all approach (antibiotics) to a condition that requires category-specific treatment.
The most important thing I do for a man presenting with prostatitis is establish which type he has. The treatment differs completely depending on the category — and most men have been treated for the wrong one.— Dr Kishore Bahl
NIH Classification
The Four Categories of Prostatitis
The NIH classification system divides prostatitis into four categories. Dr Bahl assesses all four — establishing the correct diagnosis before recommending treatment.
Category I
Acute Bacterial Prostatitis
A sudden bacterial infection of the prostate. Typically presents with fever, severe pelvic pain, urinary symptoms, and systemic illness. Requires urgent antibiotic treatment. Uncommon — accounts for less than 5% of prostatitis diagnoses.
Treatment: Appropriate antibiotic course prescribed following assessment and culture results.
Category II
Chronic Bacterial Prostatitis
Recurring bacterial infection of the prostate. Symptoms come and go — recurrent urinary tract infections, pelvic discomfort, and urinary symptoms. Confirmed by bacterial cultures of prostatic fluid. Less common than Category III.
Treatment: Prolonged antibiotic course (typically 4-6 weeks) with appropriate agent based on culture sensitivity.
Category III
Chronic Pelvic Pain Syndrome (CPPS)
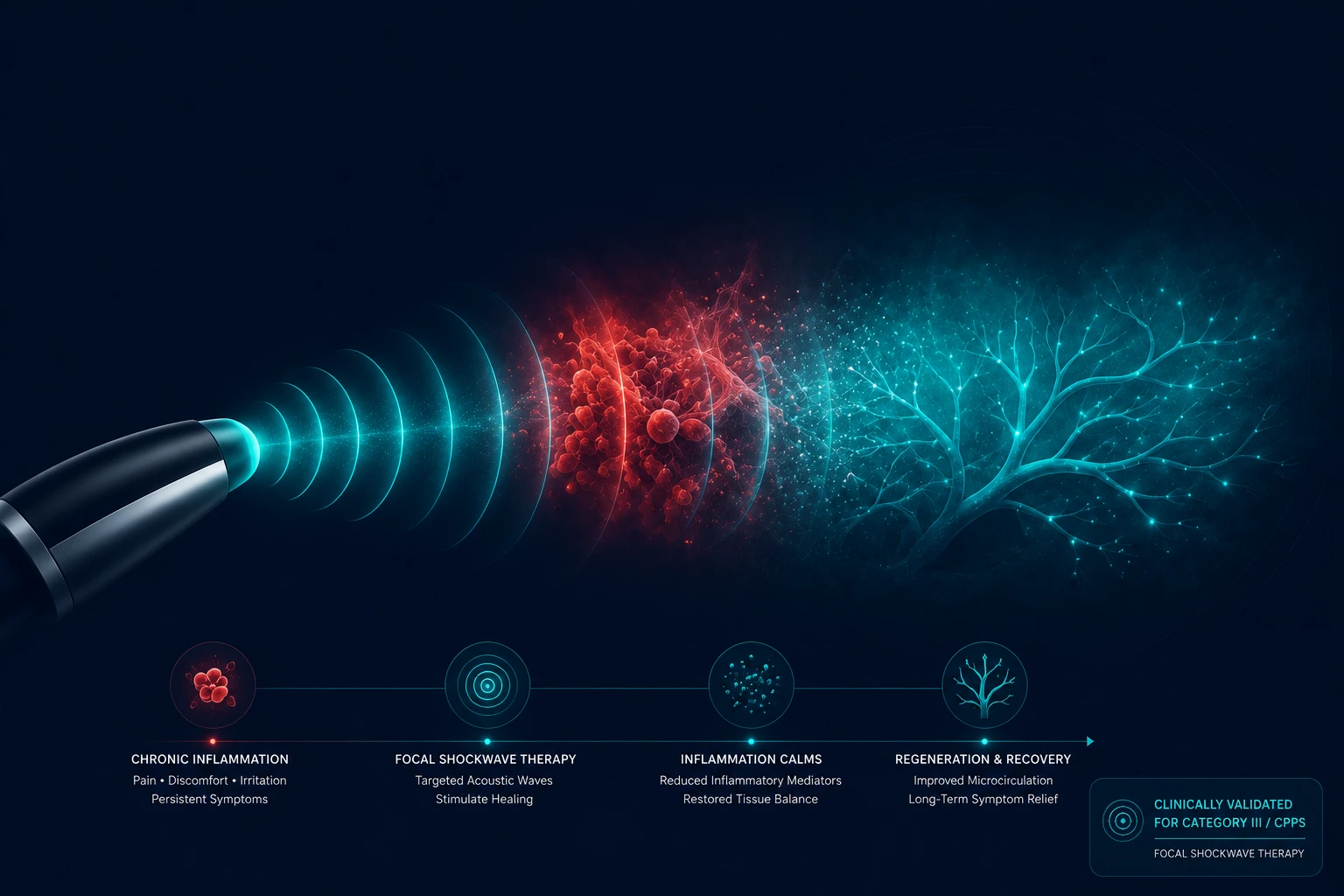
Chronic pelvic pain lasting more than 3 months without bacterial infection. Accounts for approximately 90% of all prostatitis diagnoses. Antibiotics are ineffective — yet this is the most commonly prescribed treatment. Focal shockwave therapy is the clinically validated intervention for Category III.
Treatment: Focal shockwave therapy — 78% improvement rate in published RCT (Zimmermann 2018). Non-invasive, drug-free, no downtime.
Learn more about shockwave therapy for CPPS →Category IV
Asymptomatic Inflammatory Prostatitis
Prostate inflammation found incidentally during investigation for other conditions (e.g. elevated PSA, infertility workup). The patient has no symptoms. Typically requires no active treatment but should be monitored.
Treatment: Monitoring and investigation of the underlying reason for discovery. Management depends on clinical context.
Recognising the Symptoms
Symptoms of Prostatitis
Prostatitis symptoms vary depending on the category. Acute bacterial prostatitis (Category I) is usually unmistakable — sudden onset with systemic illness. Chronic prostatitis / CPPS (Category III) is often more subtle and gradual.
Common Across Categories
- Pelvic pain or discomfort
- Pain in the perineum (between scrotum and anus)
- Lower abdominal or suprapubic pain
- Urinary urgency and frequency
- Difficulty or pain when urinating
- Incomplete bladder emptying
- Pain or burning during urination
Chronic Prostatitis / CPPS Specific
- Pain lasting more than 3 months
- Pain during or after ejaculation
- Testicular or scrotal discomfort
- Pain on sitting for extended periods
- Lower back pain without spinal cause
- Sexual dysfunction (ED, PE)
- Fatigue and reduced quality of life
- Anxiety and depression secondary to chronic pain
If you have been prescribed multiple courses of antibiotics without lasting improvement, Category III (CPPS) is the most likely diagnosis. This is the category for which focal shockwave therapy is clinically validated.
The Most Common Mistake
Why Antibiotics Don't Work for Most Men With Prostatitis
The single most common reason men with prostatitis do not improve is being treated with antibiotics for a non-bacterial condition. Category III prostatitis — which accounts for 90% of all prostatitis diagnoses — is not caused by bacterial infection. There is no bacterial target for antibiotics to address.
Despite this, antibiotics are routinely prescribed as a first (and often repeated) treatment for prostatitis because the symptoms overlap with bacterial infection and because many practitioners do not perform the diagnostic workup needed to distinguish between categories. The result is months or years of ineffective treatment, significant antibiotic exposure, and no improvement.
If you have had multiple courses of antibiotics for prostatitis without lasting improvement — and your urine cultures have come back negative — you almost certainly have Category III (CPPS). The correct next step is a specialist urology assessment, not another antibiotic.
of prostatitis diagnoses are Category III (CPPS) — not bacterial. Antibiotics are ineffective for this category.
The Treatment
Focal Shockwave Therapy for Chronic Prostatitis (Category III)
For Category III prostatitis (CPPS), focal shockwave therapy is the most clinically validated non-invasive treatment available. It delivers precisely targeted acoustic energy waves to the pelvic region — stimulating biological repair mechanisms, promoting new blood vessel formation, reducing inflammation, and breaking down trigger points in the pelvic floor musculature.
The Clinical Evidence
A 2018 randomised controlled trial (Zimmermann et al.) demonstrated that 78% of patients receiving focal shockwave therapy for Category III prostatitis achieved clinically significant improvement in NIH-CPSI scores. The treatment was well tolerated with no serious adverse events. Results were sustained at follow-up.
Treatment Protocol
- Typically 6-8 sessions
- Delivered weekly or bi-weekly
- Each session approximately 20-30 minutes
- No anaesthesia required
- No downtime — return to normal activity immediately
- NIH-CPSI score tracked throughout to measure improvement objectively
Shockwave ReVibe Clinic uses true focal shockwave technology — the device validated in the published clinical studies. Radial devices cannot achieve the penetration depth required for pelvic treatment and are not validated for prostatitis. Dr Bahl uses only focal shockwave.
Why Shockwave ReVibe Clinic
Built on Precision, Evidence and Specialist Care
Correct Diagnosis First
The most important step in prostatitis management is establishing which category you have. Dr Bahl's specialist assessment — not a 10-minute GP appointment — provides the thorough evaluation needed to make this distinction correctly.
Focal Shockwave — Not Radial
Shockwave ReVibe Clinic uses true focal shockwave technology, validated in the published CPPS clinical trials. Radial devices are not appropriate for pelvic treatment and are not validated for prostatitis. The distinction matters clinically.
Specialist Urologist
Prostatitis is a urological condition. Dr Bahl is a Specialist Grade Doctor in Urology with 15 years of specialist experience. Every consultation and treatment is delivered personally by Dr Bahl — no delegation.
Beyond Antibiotics
For Category III (CPPS) — the most common type — Dr Bahl offers the clinically validated alternative to repeated ineffective antibiotic courses: focal shockwave therapy with a 78% published improvement rate.

Prostatitis is one of the most common diagnoses in urology — and one of the most consistently mismanaged. Most of the men I see have already had multiple rounds of antibiotics before anyone stopped to ask which type of prostatitis they actually have.

Got questions?
Frequently Asked Questions
Stop Treating the Wrong Thing.
A specialist urology assessment with Dr Kishore Bahl — establishing the correct diagnosis and delivering the clinically appropriate treatment. No referral needed.
📍 22 Notting Hill Gate, London W11 3JE · GMC-registered Urologist · No referral needed
Prefer a broader assessment? Start with a Men's Urology Consultation.
By booking an appointment you agree to our Privacy Policy
Find Us on Google
Share your experience — your review helps others find our clinic.